

A torn seam on a medical gown goes beyond a small mistake. It creates a massive safety risk. Buyers pick out disposable gowns for busy hospitals every day. Often, they ignore the seam construction. We must close this awareness gap.
So, should you choose traditional sewing or ultrasonic sealing? Your budget and required protection levels drive this choice. Consider the specific fluids hitting that seam during a procedure. These details matter. They create a huge impact in real hospital settings.
Both methods play a major role in isolation gown manufacturing . Makers have relied on them for years. But they handle fluid pressure and body movements in distinct ways. They also pass strict safety tests with unique results. The actual performance gap is huge. It surprises most buyers.
Let’s review both options. This breakdown helps you pick the proper seam type. You get exact answers for your specific needs. It removes the guesswork from your next order.
What Makes a Disposable Gown Seam “Good Enough”?
 There’s a number: 7 lbf (≈31 N).
There’s a number: 7 lbf (≈31 N).
That’s the minimum seam strength threshold under ASTM F2407 for medical gowns. Some disposable gowns on the market just barely clear it. Reusable gowns tend to land well above that floor. The gap looks small on paper. In a Level 3 surgical environment, it’s not small at all.
Raw tensile strength is just one piece of the picture. AAMI PB70 adds a requirement that many procurement specs miss: every seam in a critical zone must match the liquid barrier rating of the surrounding fabric. A Level 3-rated chest panel paired with an untested seam is not a Level 3 gown. It’s a Level 3 gown with an unverified weak point.
ECRI states it directly: seams and tie attachment sites are the first places to fail under hydrostatic pressure. Not the fabric. The seam.
Three performance properties define whether a seam holds:
- Fluid barrier integrity — does it pass AATCC TM 127 hydrostatic testing at the seam , not just on a flat swatch?
- Particle shedding — does the seam construction (stitched vs. sealed) expose raw fiber edges that shed lint into sterile fields?
- Structural integrity under doffing stress — a clinician breaks the back tie. Does the gown release clean? Or does it split along the shoulder seam and drag contamination with it?
That last failure mode is what ECRI calls an ” insidious danger ” — invisible until it matters most.
How Sewn Seams Work in Disposable Gowns Manufacturing?
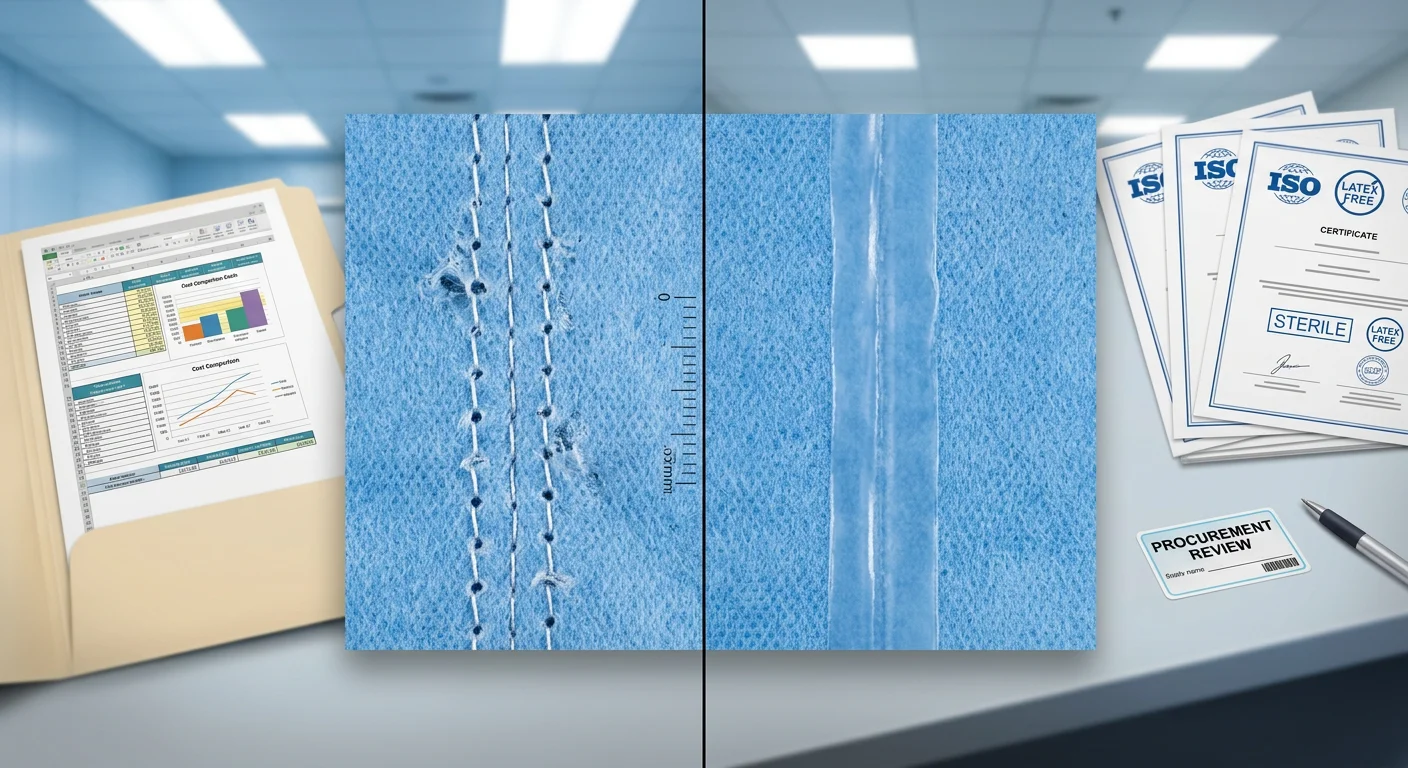
 Every time a needle punches through non-woven fabric, it leaves something behind: a hole.
Every time a needle punches through non-woven fabric, it leaves something behind: a hole.
That’s not a flaw in execution — it’s physics. The needle pierces the material. The thread passes through. A small open channel stays behind. In woven textiles, surrounding fibers can close around that puncture. In SMS fabric medical gowns , that doesn’t happen. The spunbond-meltblown-spunbond structure gets compressed, torn, and punched through at each stitch point. The meltblown filtration layer — the layer doing the real barrier work — takes damage at every single needle hole.
Here’s the mechanical reality: liquid doesn’t need to blast through a seam all at once. It finds the needle hole, follows the thread gap, hits the next needle hole, and chains its way through. That’s not a theoretical failure mode. That’s how seam integrity breaks down under fluid pressure in real conditions.
Where Stitching Still Has a Role?
Sewn seams aren’t the wrong choice for disposable gown construction across the board — they’re just wrong in the wrong zones.
Lockstitch works well for structural joining in low-exposure areas. Overlock and serged edges handle non-critical perimeters without issue. But neither stitch type acts as a fluid barrier on its own. In AAMI-rated barrier protection gowns, the critical exposure zone — front chest to knee, sleeve cuff to elbow — needs more than thread.
The industry reflects this clearly: stitching handles structure; sealing handles protection. Manufacturers who ignore that split end up with a gown that passes tensile testing and fails hydrostatic pressure testing right at the seam line. Tighter stitching won’t fix it. The real fix is tape sealing or thermal bonding applied over the stitch — a secondary closure that physically seals the needle-hole chain shut.
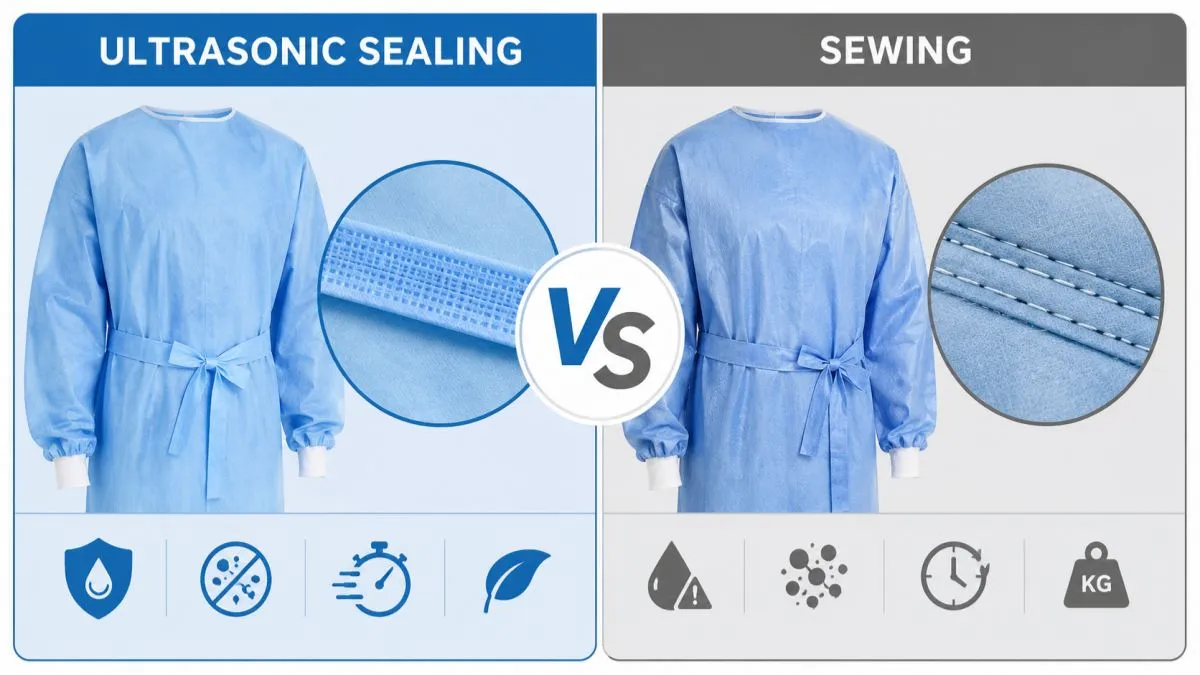
How Ultrasonic Sealing Works in Disposable Gowns Construction?
No thread. No needle. No holes. That’s the entire point.
Ultrasonic sealing bonds non-woven fabric gowns by vibrating the material into a molten state. It then cools into a continuous, pore-free joint. Here’s how it works: a generator outputs a high-frequency electrical signal at 20–35 kHz. A transducer converts that into mechanical vibration. Then a welding horn (sonotrode) drives those micro-oscillations — amplitudes of just 10–50 μm — into the fabric stack.
The real action happens at the anvil wheel below.
That rotating wheel has a patterned surface — raised dots or ridges. This concentrates mechanical energy into precise, controlled zones. Where horn meets anvil, Polypropylene fibers in the SMS fabric generate rapid intermolecular friction. Local temperatures spike past PP’s melting point of 160–165°C in milliseconds. Fiber surfaces liquefy and flow into adjacent layers. They then re-crystallize under sustained pressure into what the industry calls a molecular-level fusion bond.
The result isn’t a seam in the traditional sense. It’s a structural bridge built from the gown’s own polymer — no foreign thread, no puncture channels, no residual lint.
A few things worth noting for procurement specs:
- Weld strength matches or exceeds base fabric strength. Under tensile load, failure occurs in the surrounding material — not the weld zone itself
- Production speed in continuous bonding mode can reach 800 m/min. Critical seam zones on barrier protection gowns (sleeve cuffs, side seams) run at slower speeds to maintain tighter seal integrity
- SMS and SMMS constructions — the dominant materials in isolation gown manufacturing — work naturally with this process. All thermoplastic PP/PE layers, including the interior meltblown filtration layer, take part in the fusion bond
That last point matters more than it sounds. The meltblown layer is the barrier. With ultrasonic sealing, the bond includes that layer — it doesn’t punch through it.
Ultrasonic Sealing Vs Sewing: 8 Critical Dimensions Compared
 Eight dimensions. One clear verdict per row. Here’s what the data shows when you put both seam types side by side across the criteria that matter in clinical and procurement decisions.
Eight dimensions. One clear verdict per row. Here’s what the data shows when you put both seam types side by side across the criteria that matter in clinical and procurement decisions.
1. Fluid Barrier Integrity
Needle holes don’t close in SMS fabric. Each puncture — 80–120 μm in diameter — creates a capillary channel. Without seam tape, synthetic blood penetrates those channels at hydrostatic pressure as low as 1 . 75–3.5 kPa. That’s not much pressure. A surgeon leaning into a table generates more.
Ultrasonic-welded seams have no holes at all. At 2 psi (≈13.8 kPa) of synthetic blood pressure, the tested samples showed zero penetration across 32 specimens at AQL 0.65. That’s more than three times the pressure level where stitched seams start failing without tape. The weld geometry that removes needle holes also lifts the barrier classification by one full level under EN 14126 — from Class 3 to Class 4–5 in documented engineering practice.
Advantage: Ultrasonic sealing — by a clear margin.
2. Seam Strength
The result here surprises most buyers. On identical fabric weights, ultrasonic and reinforced sewn seams perform in the same range.
- Typical three-thread overlock on non-woven PPE gowns: 80–150 N/5 cm
- Add a heat-sealed tape strip: 120–200 N/5 cm
- Ultrasonic weld at 10–12 mm width: 150–220 N/5 cm
At the ultrasonic weld range, failure shifts to the base fabric — not the weld zone. That’s the same “fabric-dominant failure” mode you see in high-density lockstitch at 6 stitches/cm.
Neither method is fragile. The seam strength gap is smaller than most procurement specs assume.
Advantage: Close to equal in high-quality execution. Ultrasonic edges are ahead at the top of the range.
3. Particle Shedding
EN 13795 sets the acceptable threshold for cleanable particles (≥0.5 μm) at 3,500–4,000 particles/m³ for high-performance surgical gowns . The standard also flags seams and cut edges — not fabric panels — as the main contamination sites.
Stitched seams shed a lot. Thread tails, back-tack buildup, and exposed fiber edges at stitch points all contribute. Research shows that seam thread alone accounts for 15–30% of the total particle count in surgical gown evaluations. Multifilament polyester thread gets worse with repeated flexion — it pills, sheds, and adds to the ≥5 μm count that matters most in sterile fields.
Ultrasonic bonding removes the thread entirely. Same base fabric, no visible seam thread, less cut exposure. The result: 20–40% lower total particle shedding versus stitched equivalents. Top manufacturers supplying ISO Class 5–7 cleanroom environments now treat full ultrasonic welding of critical zones as standard — not a premium add-on.
Advantage: Ultrasonic sealing.
4. Comfort and Fit
Stitched seams on 50–80 GSM non-woven PPE build up to 0.6–0.9 mm at the fold, two to three times the base fabric thickness. Bending stiffness at the seam rises by 30–60% over the surrounding material. Over a four-hour procedure, that ridge at the shoulder or elbow becomes noticeable.
Ultrasonic welds on the same material measure 0.3–0.5 mm thick. Bending stiffness rises by just 10–25%, with a smooth outer surface. The tactile difference is real and measurable — not marketing language.
Dimensional stability is another gap. Stitched seams stretch under sustained load. Sleeve and body length can drift ±1–2 cm as needle holes widen and the thread elongates. Ultrasonic seam length is die- and wheel-controlled. In automated production, dimensional variance holds to ±1–2 mm. For consistent sizing across large clinical orders, that’s a spec worth caring about.
Advantage: Ultrasonic sealing.
5. Production Consistency
Human sewers are skilled. They’re also variable. Internal OEM defect data for isolation gown manufacturing puts stitch-related defects — skipped stitches, thread breaks, seam misalignment — at 3–8% of total rejects in labor-intensive lines. A well-run manual line hits 90–95% yield, with per-worker output around 250–350 units per shift.
Automated ultrasonic lines pull shoulder seams, side seams, cuffs, and hood attachment into one guided continuous process. Typical yield: ≥97–99%. Inline vision and pressure sensors catch weld defects before they reach packing. Output per equivalent staffing level: 600–900 units per shift, with seam strength and dimensional variance held within ±5% across shifts.
Advantage: Ultrasonic sealing — by a wide margin.
6. Material Compatibility
This is where stitching holds its ground. Needle-and-thread works on nearly every sewable substrate — cotton, poly-cotton, viscose, non-thermoplastic blends. Mechanical penetration doesn’t depend on melting point.
Ultrasonic welding needs thermoplastic content. 100% PP, PET, PA — no issue. Cotton-rich blends are a different story. Weld strength drops to 40–60% of the thermoplastic baseline without a thermoplastic interface layer or welding strip at the seam zone. For standard SMS fabric medical gowns and PP/PE composites, that’s not a constraint. For specialty garments that include natural fiber layers, it is.
Advantage: Sewn seams for mixed-fiber applications. Ultrasonic for thermoplastic-dominant substrates.
7. Equipment and Per-Unit Cost
The upfront numbers favor stitching. Industrial lockstitch and overlock machines cost around 20–40% of a comparable ultrasonic welding unit. Per-unit consumable cost for sewn disposable gowns: $0.01–0.03 in thread and needles. Ultrasonic equipment consumables are low — sonotrode and transducer wear over time, with no thread stock to manage.
The picture flips at scale. Labor cost per unit on manual lines is higher by design. Ultrasonic lines run with fewer operators per unit of output. They cut defect-related rework costs and don’t need seam tape as a secondary barrier step, which is a real material and labor cost in sewn barrier protection gown production.
Advantage: Sewn for low-volume or low-capex contexts. Ultrasonic wins on per-unit economics at scale.
8. Regulatory and Standards Alignment
Both construction methods can produce gowns that pass AAMI PB70, EN 13795, and FDA 510(k) requirements — but the compliance path looks different.
Sewn seams need seam tape over critical zones to hit the hydrostatic pressure requirements for Level 3–4 fluid resistance surgical gown construction. The tape adds cost, adds a process step, and adds a potential delamination failure point. Without it, a sewn seam can’t match the barrier rating of the surrounding panel in a Level 3+ gown. That means the gown fails AAMI PB70’s zone-matching requirement regardless of fabric rating.
Ultrasonic-bonded stitch-free seam technology meets critical-zone barrier requirements in a single step. No secondary tape needed. The weld is the barrier — same PP matrix as the base fabric, continuous and pore-free. That cuts compliance documentation and reduces the process variables a quality engineer has to control and validate.
Advantage: Ultrasonic sealing for Level 3–4 clinical environments. Sewn with tape for Level 1–2 where cost is the dominant factor.
Which Seam Is Right for Your Use Case?
 Stop optimizing for the seam. Start optimizing for the room.
Stop optimizing for the seam. Start optimizing for the room.
A surgical gown seam for an orthopedic OR is not the same as an isolation gown seam for a general ward. Treating them as the same thing is how procurement decisions create infection risk. The framework below cuts straight to the match.
Operating Room (AAMI Level 3–4)
Full ultrasonic welding across all critical zones — front chest, sleeves, forearms — is the standard here. For high-splash procedures like trauma or orthopedic surgery, add taped seams over welded construction. That closes the remaining gap. Sewn seams, even reinforced ones, cannot pass ASTM F1671 viral penetration testing at critical locations. Without a continuous sealed layer, every needle hole becomes a channel for contamination.
ICU (AAMI Level 2–3)
A shift that includes intubation, suctioning, or high-volume fluid exposure calls for OR-level seam standards. Use ultrasonic or bound-plus-tape seams on the front chest and sleeve cuffs. For general monitoring and routine care, standard serged construction is enough. Level 2 fabric handles the job where splash risk stays low.
General Isolation Wards and Outpatient Clinics (AAMI Level 1–2)
Three-to-five thread serged seams or lockstitch with binding work well here. No ultrasonic bonding needed. The trigger to upgrade is frequency. High-flow oxygen therapy or repeated fluid exposure becoming routine in that space? Move up one level and review the seam spec.
The Purchasing Priority Filter
| Priority | Minimum Seam Requirement | Typical FOB Range |
|---|---|---|
| Cost-first | Serged/lockstitch, Level 1–2 | $0.25–0.50/unit |
| Compliance-first | Ultrasonic or taped, Level 3–4 critical zones | $0.80–1.50/unit |
| Infection control-first | Ultrasonic + tape, Level 4, batch seam retesting | $1.50–3.00+/unit |
One step every procurement spec should include: request seam-specific test reports, not just fabric swatch data. AATCC 127 hydrostatic results on a flat panel tell you nothing about the sleeve seam under pressure; where the sample comes from matters just as much as the number on the report.
Conclusion
The seam holding your gown together stands between your patient and a preventable infection. That’s not dramatic — that’s just physics.
Here’s what this comparison guide makes clear: sewn seams and ultrasonic sealing are not interchangeable. They are different answers to different questions.
- Low-acuity isolation settings: Traditional stitching still delivers solid performance at a lower cost.
- Surgical environments or fluid-intensive procedures: Ultrasonic sealing isn’t a premium upgrade. It’s the baseline requirement — especially where barrier protection gowns must meet AAMI Level 3–4 or EN 13795 High Performance standards.
Know your use case. Match your seam technology to it. Then buy what fits that need.
Ready to check your current gown supplier’s seam specs? Request a sample or technical data sheet from our team — because the right question to ask your vendor isn’t “how much?” It’s “how does that seam hold under pressure?”