

Choosing between Halyard’s AERO and ULTRA isn’t a catalog decision — it’s a scrubbed-in one. Most procurement guides hand you a spec sheet and stop there. Spec sheets don’t sweat through a six-hour spinal fusion. They don’t tell you what happens when fluid hits a reinforced panel at the wrong angle in hour three.
This comparison is built on real OR conditions. It’s structured around the moments that matter most during surgery — not marketing language.
Evaluating Halyard surgical gowns for a high-volume trauma program? Trying to match the right AAMI Level 4 surgical gown to the right procedure? Either way, what follows gives you the clarity that product datasheets fail to deliver.
What You Notice First: AERO vs ULTRA in Real Surgery
 The difference hits you before the first incision closes.
The difference hits you before the first incision closes.
Scrub techs who’ve worked with both Halyard surgical gowns say the same thing: the ULTRA feels heavier before you even tie in. That weight is intentional. The reinforced panels are thicker across the chest, the forearms, and the critical fluid-strike zones. They’re built for procedures where fluid exposure isn’t a possibility. It’s a certainty.
The AERO feels different. Lighter. It moves with your arms during fine work. Two hours in, repositioning again and again — that flexibility matters more than most procurement specs admit.
Here’s what the spec sheet won’t tell you:
- Fluid behavior at the reinforced panel — Under sustained fluid pressure, the ULTRA’s AAMI Level 4 barrier holds. The AERO carries a lower rating. It handles moderate fluid exposure well, but shows real limits when saturation runs long or hits from a specific direction.
- Thermal load — The AERO’s surgical gown breathability edge shows up after the 90-minute mark. In longer cases, managing core temperature is a real clinical factor. It’s not just a comfort preference.
- Mobility under a reinforced gown — ULTRA’s reinforced surgical gown design gives up some range of motion for stronger barrier protection. Most surgeons adapt fast. Some never quite get there.
These aren’t abstract observations. Experienced OR teams notice these things right away — and these are exactly the factors that should drive your choice between these two disposable surgical gowns.
After 1–2 Hours: Where Halyard AERO Starts to Feel Different
 Ninety minutes into a long case, something shifts.
Ninety minutes into a long case, something shifts.
It’s not dramatic. There’s no single moment where the Halyard AERO announces itself. It’s more of a slow realization — the kind that creeps up on you between retractor holds and instrument passes. The gown stops feeling like something you’re wearing. It starts feeling like something is working with you.
That’s the AERO’s real story. It only makes sense in real time.
The Thermal Tipping Point
Surgical gown breathability doesn’t matter — until it does. For the first hour, most gowns feel about the same. Your core temperature is still manageable. The OR is climate-controlled. The Halyard ULTRA’s reinforced panels feel secure, not restrictive.
Then hour two arrives.
The thermal load that’s been building starts to matter. Surgeons in ULTRA gowns during extended procedures — complex orthopedic cases, long vascular reconstructions, multi-stage oncology resections — report the same pattern. Heat builds across the chest and forearms. Tension creeps into the shoulders. The gown itself enters your awareness.
The Halyard AERO’s lighter build pushes that threshold back. It doesn’t eliminate heat buildup. But in a four-hour procedure, delaying the tipping point is a real clinical difference — not just a comfort preference.
Mobility Compounds Over Time
Early in a case, the range-of-motion gap between the two gowns feels small. Most surgeons adjust to the ULTRA’s stiffer panels within the first twenty minutes. It’s manageable.
Over time, that changes.
Repetitive overhead work. Sustained lateral reach. Fine microsurgical movements are repeated dozens of times. The AERO’s flexibility edge isn’t about one gesture — it’s about cumulative physical demand across hundreds of small movements. Scrub technicians and surgical nurses who’ve run long cases in both gowns describe the same thing: the ULTRA becomes something you’re working against. It happens bit by bit. You don’t notice it — until you do, all at once.
Halyard ULTRA: Where It Works — And Where It Doesn’t
 Some procedures make the Halyard ULTRA feel like the obvious choice, not a compromise.
Some procedures make the Halyard ULTRA feel like the obvious choice, not a compromise.
Short cases. High fluid volume. Emergency laparotomies. Ruptured ectopic pregnancies. Trauma damage control surgery where blood loss hits fast and unpredictably. In these situations, the ULTRA’s AAMI Level 4 surgical gown rating isn’t just a spec on paper — it’s the whole point. The reinforced chest and forearm panels block what the AERO can’t. The barrier holds under pressure that would breach a lower-rated fluid-resistant surgical gown before the second instrument pass.
Surgeons in high-acuity, short-duration trauma cases tend to reach for the ULTRA. They’re not in the OR long enough for heat to build up. Mobility trade-offs don’t pile up when you’re closing in under ninety minutes. The weight feels solid, not heavy. Those thicker panels feel like armor — because in those moments, that’s what they are.
That’s where the ULTRA earns its place, no debate needed.
Where the Risk Comes In?
The Halyard ULTRA isn’t the problem. The problem is applying the same logic to the wrong case.
A four-hour colorectal resection. A hepatobiliary procedure. A staged reconstructive case that runs long — because they always do. Fluid exposure in these cases is real, but not overwhelming. The surgical gown barrier protection the ULTRA provides matters, but it’s not the only option that works. These are the cases where the ULTRA’s weight and reduced breathability start working against the surgeon.
Heat builds. The reinforced panels stiffen as fatigue sets in. What felt like security in hour one starts feeling like friction in hour three. The gown pulls at the surgeon’s attention at the worst possible moment — deep in a complex dissection, needing full focus on tissue planes and anatomy, not on managing discomfort inside a sterile field gown that’s pushing back.
This isn’t a hypothetical. OR teams running extended cases report it. The Halyard ULTRA wasn’t built to carry a surgeon through a marathon. It was built for acute, high-intensity fluid exposure — and then it should come off.
The Moment You Realize You Chose the Wrong Halyard Surgical Gown
It doesn’t announce itself. That’s the thing nobody tells you.
There’s no alarm. No visible breach. No single moment where the gown fails, and you know it. The realization creeps in — slow and quiet, the way fatigue does. You’re two hours into a hepatobiliary case. You’ve repositioned three times. The reinforced panels feel stiffer than at the start. A low-grade heat has settled across your chest and forearms. Your focus is on the tissue plane, on the dissection — but something at the edge of your awareness keeps pulling.
That’s it. That’s the moment.
Not a catastrophic fluid breach. There is no visible tear in the sterile field gown. Just the gown, announcing itself at the worst possible time.
The Wrong Halyard Surgical Gown in the Wrong Case
The mismatch starts before the first incision. Some teams default to the ULTRA for every procedure. It carries AAMI Level 4 protection — and higher feels safer, right? That decision will cost them in hour three. The reinforced surgical gown was the right call for yesterday’s emergency laparotomy. It’s not the right call for today’s four-hour colorectal resection.
The reverse happens too. An AERO in a high-acuity trauma case where fluid exposure hits fast and hard. The fluid-resistant surgical gown rating looked fine on the spec sheet. Then, sustained pressure hits the critical zones. The limits show up fast. There’s no clean way to recover from that inside a sterile field.
Both are procurement errors dressed up as clinical ones.
What the Wrong Choice Costs
The cost isn’t a contamination event most of the time. That’s a rare worst case. The real cost builds quietly:
- Surgeon fatigue sets in earlier than it should — the gown is working against the body, not with it
- Compromised focus during the deep, demanding phases of a long case — surgical gown breathability failures pile up into a distraction
- Infection control risk rises not from one failure, but from a surgeon working at reduced capacity inside the wrong operating room gown
Wrong-gown realizations don’t make it into incident reports. They stay in the OR — in the shrug after a long case, in the scrub tech’s quiet note to herself, in the surgeon who can’t name what felt off but knows something did.
The spec sheet never captures any of that. The procedure does.
A Simple Way to Choose (Without Overthinking)
 Three questions. That’s all this takes.
Three questions. That’s all this takes.
You’ve read through the thermal data, the fluid exposure windows, and the cumulative fatigue patterns. It’s tempting to build a spreadsheet. Run a scoring matrix. Get a committee involved. But committee-driven procurement tends to land on the safest-looking answer — not the most useful one.
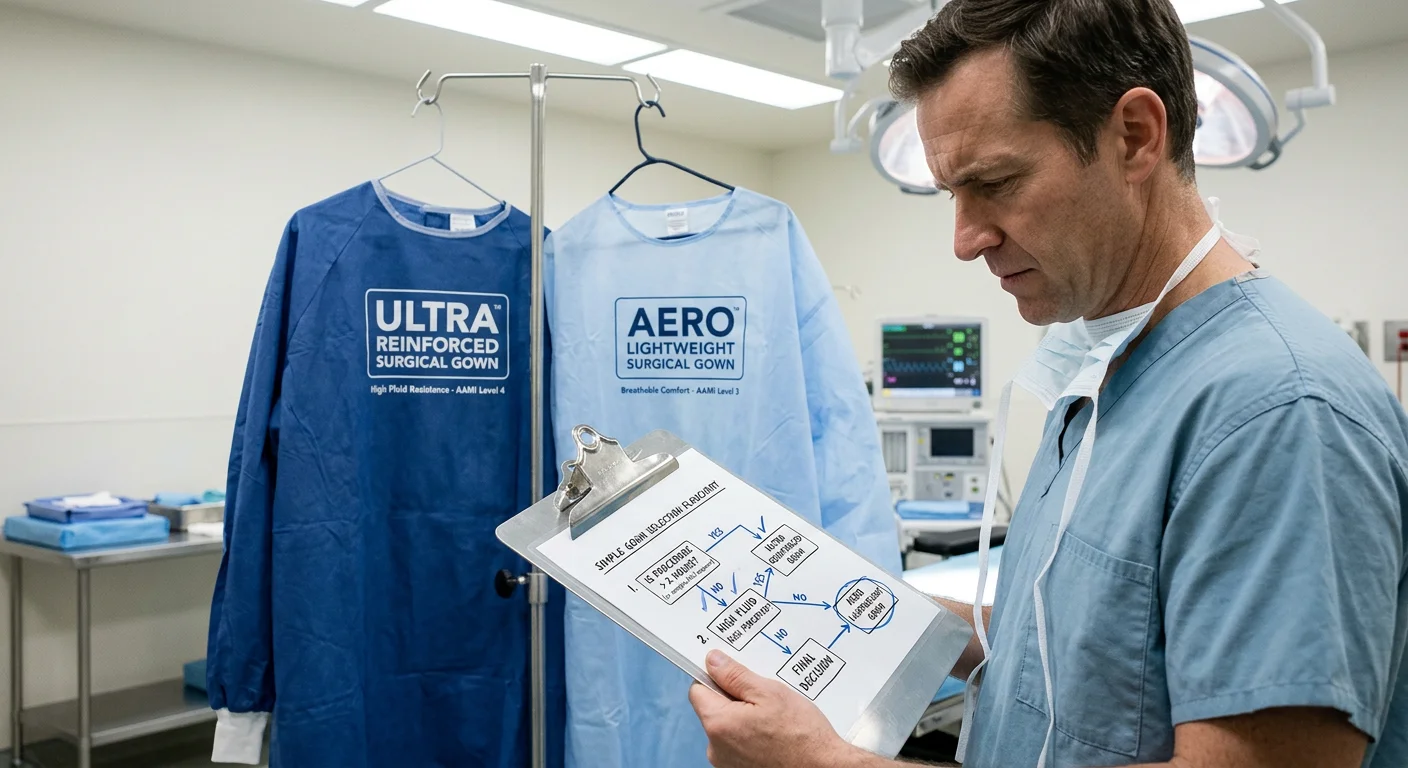
Here’s the decision framework that works in practice:
1. How long is the case?
Under 90 minutes: ULTRA. Over two hours: AERO. That one variable cuts through most of the confusion before anything else comes into play.
2. What’s the realistic fluid exposure?
Not the worst-case scenario. The realistic one.
- Emergency laparotomy, ruptured ectopic, high-volume trauma — ULTRA’s AAMI Level 4 surgical gown barrier is the right call. It’s not a close comparison.
- Moderate fluid exposure across a long resection — the fluid-resistant surgical gown rating on the AERO covers the real case, not the imagined one.
3. What happens if you’re wrong?
– An AERO in a low-acuity long case: manageable.
– An AERO in a high-acuity, fluid-heavy case: a real problem.
– An ULTRA in a short, high-risk case: the right choice.
– An ULTRA in a four-hour procedure: the surgeon feels it in hour three.
The asymmetry is real. Errors in one direction carry clinical risk. Errors in the other direction carry performance cost. Both matter in a sterile field gown decision.
The Default Trap
Most programs default to one gown. It feels efficient. It keeps inventory simple. It removes the decision from the table — and that’s the problem.
No decision is still a decision. A single-gown protocol built around your highest-acuity cases will fall short in your longest ones. The reverse is just as true.
Stock both. Use the three questions. The answer comes faster than any spec sheet review — because it’s based on the procedure in front of you, not the catalog sitting behind you.
Final Take: What I Would Choose After Using Both
Neither gown wins outright. That’s not a hedge — it’s the honest answer after using both in real conditions.
The ULTRA is my first pick for high-acuity trauma cases and emergency laparotomies. Any situation where fluid hits fast and time is short — that’s where it belongs. The AAMI Level 4 surgical gown barrier does what it promises. In those moments, that promise is everything.
The AERO is what I’d want for anything running past two hours. Not because the ULTRA fails — it doesn’t. The AERO just stops working against you as the case drags on and demands stack up. That surgical gown breathability edge isn’t a comfort bonus. It’s a performance margin. Deep into a long case, any deficit is hard to recover from.
Running a high-volume mixed surgical program? I wouldn’t pick just one for the whole catalog. That’s the wrong question. Stock both. Carrying two disposable surgical gown SKUs costs almost nothing. Fielding the wrong gown for a procedure costs far more.
The real final take: The best operating room gown is the one matched to the procedure in front of you — not the one that made it through a committee meeting.